
Foot & Ankle
Ankle Impingement
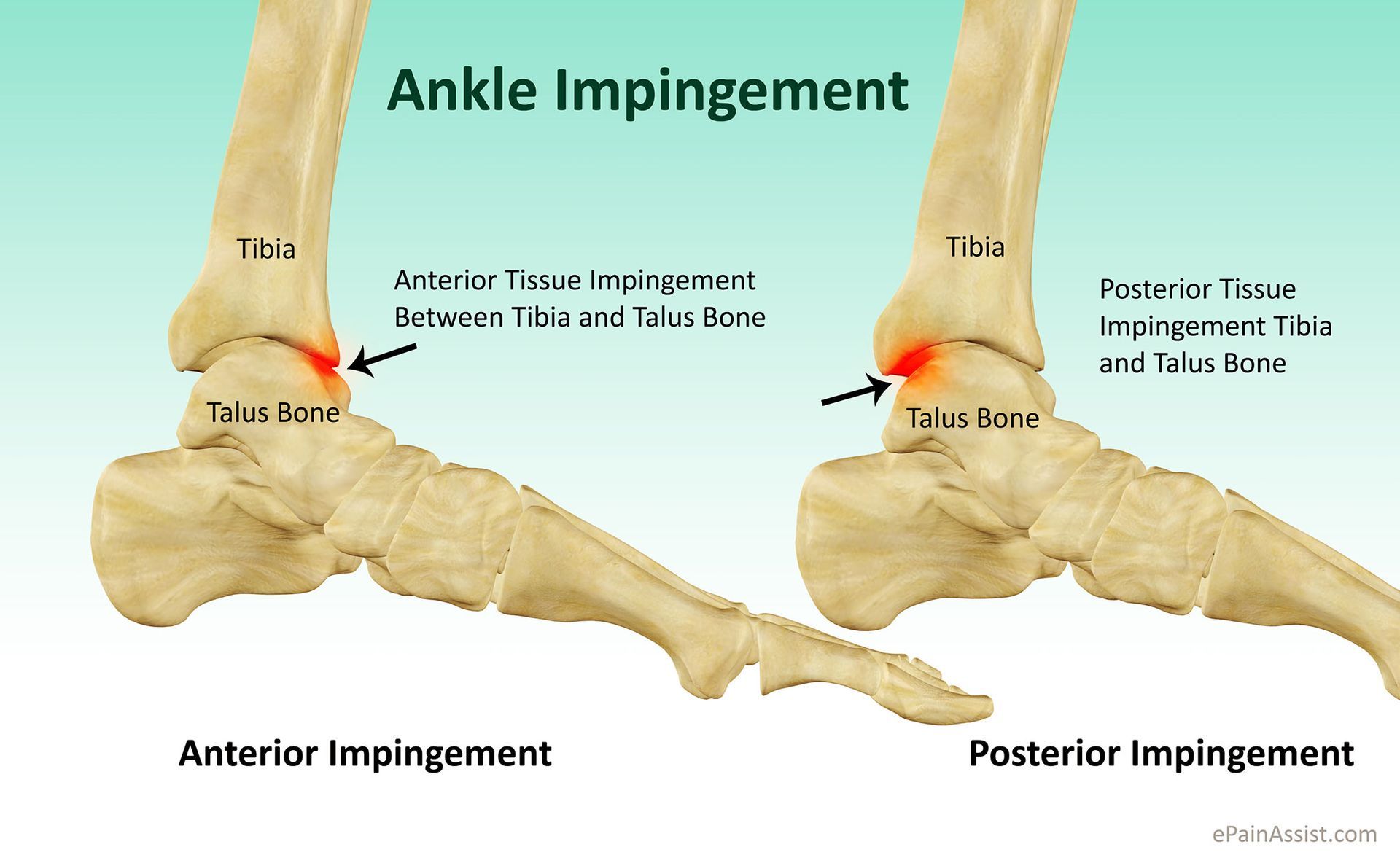
Ankle impingement is a painful condition that restricts the normal movement of the ankle joint due to an abnormality in the soft tissue or bone. This condition can occur in two main types: anterior (front) ankle impingement and posterior (back) ankle impingement.
Anterior Ankle Impingement
Anterior ankle impingement commonly affects athletes, especially those involved in sports that require repeated upward bending (dorsiflexion) of the ankle, such as football players. The repetitive movement causes irritation at the front edge of the ankle joint, which, over time, leads to impingement.
Posterior Ankle Impingement
Posterior ankle impingement is less common but seen in athletes who frequently stand on their toes or perform plantarflexion, such as ballet dancers, gymnasts, or athletes involved in jumping sports. It causes pain and swelling at the back of the ankle.
Symptoms of Ankle Impingement
The symptoms of ankle impingement vary depending on the type, but common signs include:
- Pain and swelling in the front or back of the ankle, worsening with movement
- A painful clicking sensation when twisting the foot inwards or outwards
- For anterior impingement, additional symptoms may include:
- Instability of the ankle
- Limited ankle movement
- Pain during activities like squatting, sprinting, stair climbing, and hill climbing (normal walking may not be affected)
- For posterior impingement, additional signs may include:
- Joint line tenderness in the posterior tibiotalar joint (not involving the Achilles tendon)
- Limited plantar flexion (movement of the foot downwards)
- Ligamentous instability and thickening of the soft tissue
Causes of Ankle Impingement
Ankle impingement is often caused by:
- Repetitive stress and irritation in the ankle joint
- The formation of excess scar tissue after healing from an ankle sprain
- The development of bone spurs due to continuous wear and tear
Diagnosis of Ankle Impingement
Diagnosis is made through a thorough medical consultation, including the patient's medical history and a physical examination of the ankle. A key part of the examination involves assessing the foot’s range of motion, with pain typically occurring when the tissues are pinched. To confirm the diagnosis and rule out other conditions, X-rays and bone scans may be used.
Treatment Options for Ankle Impingement
Non-Operative Treatment
Initial treatment for ankle impingement usually involves non-surgical approaches, including:
- Physiotherapy to improve ankle range of motion and break down scar tissue
- Rest and ice packs to reduce pain and inflammation
- Immobilisation using a cast or special boot to restrict movement and allow healing
- Pain relief with paracetamol (Panadol) or anti-inflammatories (if tolerated and not contraindicated)
- Corticosteroid injections may be used to reduce inflammation and provide pain relief
Surgical Treatment
If non-operative treatments are ineffective, surgical intervention may be required. Ankle arthroscopy is a minimally invasive procedure that involves excising excess scar tissue, damaged tissue, bone spurs, or other abnormalities. This approach reduces recovery time and allows for quicker rehabilitation.
Following surgery, a structured physical therapy rehabilitation programme is essential to restore strength and flexibility in the joint.
Find out more about
Ankle Arthroscopy.
Phone: (08) 9779 9767
Email: admin@ryandusart.com.au
Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Moser, M. S., et al. (2020). "Outcomes of Ankle Arthroscopy in the Treatment of Ankle Impingement Syndrome." Journal of Foot & Ankle Surgery, 59(2), 279-284.
- Bailie, G. J., et al. (2017). "A Review of the Surgical Management of Ankle Impingement." British Journal of Sports Medicine, 51(12), 938-944.
- Todhunter, R. D., et al. (2018). "Conservative and Surgical Treatment Options for Ankle Impingement Syndrome." American Journal of Orthopedics, 47(3), 174-182.
